It was recently discovered that two types of drugs significantly increase your risk of developing dementia. In two separate large population studies, both benzodiazepines (a category that includes medications for anxiety and sleeping pills) and anticholinergics (a group that encompasses medications for allergies and colds, depression, high blood pressure, and incontinence) were associated with an increased risk of dementia in people who used them for longer than a few months.
Fortunately, there are alternative treatments for all of these conditions that do not present the same dementia risks. Unfortunately, there is so much research that takes 17 years for new medical research to become common practice for physicians. For example, it was only in 1850 that it was discovered that surgeons could dramatically reduce death rates among their patients by washing their damn hands. Yet, it took over 20 years for this to become common practice.
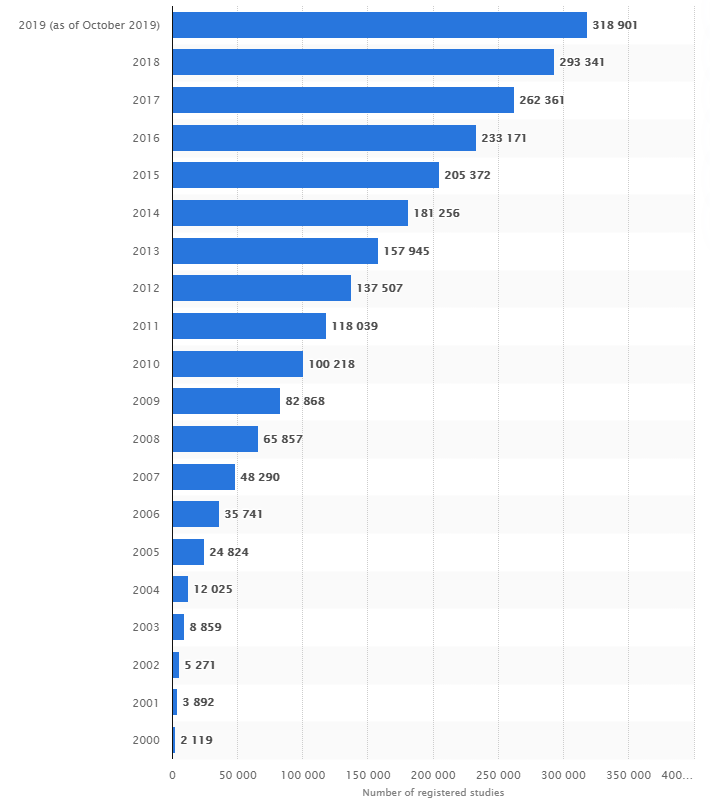
This delay is only going to get worse and worse as the amount of new research grows. In 2019, there were 205,376,752 pages of new research.
Report synopses had a median length of 5 pages, efficacy evaluation 13.5 pages, safety evaluation 17 pages, attached tables 337 pages, trial protocol 62 pages, statistical analysis plan 15 pages, and individual efficacy and safety listings had a median length of 447 and 109.5 pages, respectively. The median length of 644 pages for reports.
There is an average of 1763 words in the summary journal articles for each study. So there were 562,222,463 words in all the summarized journal articles.
The brain of a human doctor can only hold 7 numbers in working memory. In technical material, the average reading rate is approx 50 to 75 words a minute roughly 5 to 6 minutes per page.
https://bmjopen.bmj.com/content/3/2/e002496
Imagine if there were a God-like doctor that knew the results of every new research study immediately.
We consume as many as 10,000 chemicals though our diets.
We have nutrition labels that last the amount of riboflavin, but how useful is this? When one needs to hang a picture in their house, they go to the hardware store to buy a drill. However, they didn’t want the drill in itself, they just wanted the hole in their wall.
Likewise, people don’t look at nutrition labels because they want to know how much riboflavin is in it. They want to know how the food is going to impact their health.
Our goal is to have is to have Outcome Labels on the side of every food, drug, and nutritional supplement. The Outcome Labels would clearly list the percent increase of decrease in severity or onset of various symptoms of chronic illness associated with consumption of the product.
We have currently created Outcome Labels for thousands of products. However, they are currently derive from observational data donated by a small number of participants. By collecting data from more participants, we will be able to increase the precision and accuracy of these labels.